In my final year as an undergraduate at Swansea University (I graduated in July this year), I chose to write my dissertation on the relationship between the US and the Soviet Union at the United Nations Commission on Narcotic Drugs (CND) between the years 1945 and 1962. In so doing, and by utilising the online archives of the CND alongside other primary sources, the study aimed to revise and nuance the arguments of authors such as John C. McWilliams, William McAllister, Douglas Clark Kinder, Matthew Pembleton and Dave Bewley-Taylor. It was Dave, my dissertation supervisor, who suggested that I write this blog.
My interest in the topic was first piqued after reading about Harry J. Anslinger, the Commissioner of the US Federal Bureau of Narcotics (FBN) between 1930 and 1962, in Chasing the Scream: The first and Last Days of the War on Drugsby Johann Hari. Further reading about Anslinger uncovered significant anti-communist sentiment. However, a claim in a 2016 article by Mathew Pembleton suggested that there was in fact cooperation between the US and the USSR during the Cold War around anti-narcotic policy. Mindful of the tensions between the superpowers during this period, this intrigued me. I consequently emailed Professor Pembleton about the claim, and he kindly sent through some supporting primary evidence. And so began my revisionist exploration of the topic.
My research revealed that the primary foundation for cooperation between the US and the USSR between 1946 and 1950 at the fledgling CND was the personal relationship between Anslinger and the Soviet representative, Professor V.V. Zakusov. This relationship existed principally because of the flexibility of Anslinger’s pragmatic world view; a view that managed to transcend wider geopolitical tensions of the time. Such a perspective differs to that of several authors who have argued that Anslinger’s views were dominated by nationalist ideology. Instead, as primary documents reveal, Anslinger’s stance on a range of countries, including the right-wing Peru, was driven their usefulness (or otherwise) to his campaign for global drug prohibition.
Seen here, just before the start of one of the meetings of the seventh session of the Commission on Narcotic Drugs (21 April 1952), at United Nations Headquarters are (left to right) Mr. Henry J. Anslinger, delegate of the United States, Mr. John Henry Walker, representing the United Kingdom and Professor V.V. Zakusov, delegate of the U.S.S.R. Source: United Nations Photos
The importance of individual agency should come as no surprise. Indeed, during this time, but also before World War 2, there had existed a ‘heroic age’ of individuals, to use McAllister’s term. This involved personal relationships at the core of narco-diplomacy and my research argues that, while largely omitted from the current literature, the Zakusov-Anslinger relationship should be included under this heading. To be sure, despite heightened geopolitical tensions, significant cooperation existed between the US and the USSR due to their diplomat’s shared individual beliefs on international drug prohibition. Concrete cooperation came in the form of Soviet support of US proposals, and vice versa, as well as Soviet inclusions onto CND ad-hoc committees and working parties.
A significant characteristic of cooperation between 1946 and 1950 was that Soviet proposals supported by the US were largely without nationalist oriented ideological motivation. This allowed Anslinger to carefully manage tensions with the US State Department and meant that Zakusov and the Commissioner enjoyed a mutually reinforcing relationship. However, this situation changed with the establishment of the People’s Republic of China (PRC) and its exclusion from the UN. At this point, Soviet interactions at the CND became one dimensional and rigid until around 1956. Moscow’s constant protestations at the PRC’s omission was such that Zakusov’s individual agency and personal relationship with Anslinger disappeared; a dynamic that coincided with the end of the ‘heroic age.’
Another dominant argument within the wider literature on this topic challenged by my research concerns Anslinger’s treatment of the communist world as monolithic. Despite the oft given impression of the two nations as a unitary countervailing power after the Sino-Soviet alliance of 1950, Anslinger treated the PRC and the Soviet Union differently. Specific evidence for this can be seen in his briefing to several NGOs in 1957. Here he called for the Iron Curtain to be moved past the Soviet Union to China. This was due, according to the Commissioner, to the lack of Chinese cooperation compared to the ‘complete cooperation’ on drug control from the USSR.
My research also shows that some cooperation between the US and USSR did re-emerge towards the end of the 1950s and this this might be explained by two factors. First, by the mid-to-late 1950s, Nikita Khrushchev had successfully broken from Joseph Stalin’s legacy of the ‘inevitability of global war’. The Premier aimed to utilise Soviet foreign policy to generate soft power by settling disputes with opponents, as Zubok and Pleshakov have noted. It might be argued that such an approach infiltrated the realm of drug policy and the Soviet stance regarding relations with the US in the CND. Second, it is reasonable to suggest that Anslinger’s diminishing influence at the CND during this period also had a significant impact on the re-emergence of cooperation. While partly due to his strong dislike for Khrushchev, his decline is best understood as a complex mix of factors including bureaucratic infighting, the increasing influence of the more industrialised, moderate states at the CND, and the increasing pressure on him from medical professionals.
All in all, the key conclusion of my work is that the relationships that defined the ‘heroic age’ of individuals in international narco-diplomacy should include that between Zakusov and Anslinger. This relationship transcended geopolitical tensions to ensure mutually reinforcing cooperation. Indeed, it is simply incorrect to portray Anslinger as an ardent anti-communist. Rather he judged his treatment of nations at the CND on their usefulness to his global prohibitionist mission.
In a recent report for GDPO, I discussed the links between national economic models and illicit cultivation, and the way this important context has been largely ignored by the drug policy community; localised projects – amounting to rural development aid – have instead been the focus of attention. In this blog I would like to address an important but often overlooked issue: the way the proceeds from criminal activity interact with the national economic model, and vice versa. The focus will be on the kinds of “Washington Consensus” reforms that have been applied in many developing countries since the 1970s.
In 1994, the US Drug Enforcement Administration produced an interesting report on this topic, looking at the case of Colombia. The report opens with the following statement:
“Like many Latin American countries, Colombia recently has liberalized its economy through a series of reforms and relaxed import restrictions on foreign goods and services. Although Colombia may be benefiting from the resultant increase in international trade and exchange, criminal elements, including major drug kingpins, also are profiting from liberalization of the Colombian economy.”
The liberalisation of the financial services sector and the privatisation of many commercial facilities gave traffickers a new means of laundering their income. These reforms, the report notes, “will make it much more difficult for drug law enforcement officials to conduct financial investigations pertaining to drug money laundering in Colombia as well as in other countries.”Cases soon emerged of drug money being laundered through privately owned currency brokerage houses. The reforms also allowed Colombian citizens to hold dollar accounts. This meant “hundreds of millions of dollars worth of drug-related U.S. currency has been flowing into Colombia.”[1] When the government issued fixed-rate treasury securities, “these securities were sold to Colombian investors and informed sources reported that some securities were purchased with drug money.” The report comments:
Ironically, a large percentage of the foreign currency reserves that are flooding the Colombian Government’s international reserves accounts (especially the majority of U.S. dollars) are believed to stem from the repatriation of drug proceeds from U.S. and European drug markets. The revenue generated by the influx of drug proceeds into the economy has provided the Colombian Government with funds for debt payments and national infrastructure development. Furthermore, through the purchase of government-issued securities, Colombian drug kingpins are investing in their country’s future economic development.
The implications of an inflow of large amounts of US dollars could be significant, for a number of reasons. The dollar flow removes one of the persistent problems of developing countries: the shortage of foreign reserves necessary to finance imports, particularly of machinery and other capital goods needed for the development of domestic industry. Under normal circumstances, this leads to pressure to either increase exports – usually of raw materials – in order to earn the necessary currency, or to take measures to depress national demand, causing imports of consumer goods to fall (a currency devaluation, which also decreases real wages, could have such an effect).
In Colombia, the enormous amount of dollars entering the reserve accounts eliminated this balance of payments problem. In other countries, the shortage of reserves could serve as an incentive to improve the economic structure, particularly domestic export capabilities, which would create new sources of foreign exchange. In Colombia there was no such pressure. In fact, the government was able to run persistent current account deficits – imports exceeding exports – because the capital account was in surplus, thanks to the revenues from the drug trade. The DEA report refers to this as “the substitution of export revenue with revenue from illicit sources.”
In 1996, a UNODC study noted that:
In situations of reduced money growth, an infusion of hard currency can bolster a country’s foreign reserves, ease the hardship associated with expenditure-reducing policies, and moderate foreign indebtedness. Drug money could in this light be perceived as a potentially stabilizing force, a source of capital without the strings of conditionality attached … Clearly, there are “benefits” which accrue to countries which serve as reservoirs of the revenues from the international drug trade.
After the economic liberalisation in Colombia, there followed a boom in private spending – and indebtedness – and, later, government deficits. A study of this period by the Banco de la Republica, which makes no mention of illicit incomes, instead discussing “hidden capital inflows,” remarks:
Both the rapid process of fiscal deterioration and the excess of private expenditure over disposable income were greatly facilitated by huge foreign capital inflows. They allowed the economy to keep a large and increasing current account deficit of the balance of payments between 1992 and 1997. At the same time, they implied that, during most of the nineties, the foreign exchange market was characterized by excess supply of dollars and by a pressure towards a real appreciation of the Colombian peso. A vicious circle was then created. The process of appreciation of the peso promoted a further increase in expenditure and made it apparently cheaper to increase foreign indebtedness and to bring foreign assets into the country.
From a development perspective, this is a crucial issue. The demand for the domestic currency, as traffickers convert dollars into pesos, causes it to appreciate.[2] As the OAS has recognised, “The influx of large volumes of foreign exchange directed toward activities showing sudden, artificial growth could cause the currency to appreciate and produce “Dutch disease”-type consequences by making other legitimate activities less competitive.” The appreciation will make imports cheaper, but it will also mean exports are less competitive. Domestic industries, particularly manufacturing, will find it difficult to compete internationally, given the relative increase in the price of their goods. If the appreciated exchange rate persists, domestic industry could suffer significant losses. The DEA report, in fact, had observed this unfolding anti-development tendency: “The appreciation of the peso and subsequent increase in the peso’s “real value” have significantly hurt manufacturing and agricultural producers in Colombia.”[3]
In the 1990s, the appreciated peso led to inflationary pressures, and the government responded by contracting the money supply. “However, due to the constant flow of drug dollars, this action caused the value of the peso to appreciate and, in turn, domestic production costs have increased. This increase has reduced demand for export from overseas markets; at the same time, the stronger peso has increased demands for imports.”
In this sense, the presence of drug trafficking on the national territory is similar in development terms to a low-value export industry or unproductive Foreign Direct Investment (FDI): While it provides foreign reserves, the revenues are not invested in productive capacity. Drug money is traditionally laundered through real estate (a hedge against inflation), casinos, car dealerships, construction, and so on. Any associated increase in demand is consumption-based and unsustainable. Hence Medellin once experienced enormous investments in the construction sector linked to the drug trade. But once the boom subsided, the city “suffered an economic decline and high unemployment because little alternative productive investment had been made.” Similar tendencies have been noted in other regions by the UNODC:
In West Africa, in recent years, significant amounts of criminal money seems to have been invested in the construction of casinos. Recent examples of arms and drug dealers in some of the western Balkan countries revealed major investments in large-scale construction, ranging from apartment houses, shopping malls and business centres to yacht ports, officially financed by foreign banks, though with criminal funds.
These kinds of consumption patterns, created by illicit income, mimic the historic problem of Latin America: the wasteful use of much-needed foreign currency to purchase luxury goods from abroad. The DEA report, for example, found “the importation of luxury goods by Colombia and their subsequent sale has increased suspiciously by 105 percent since 1992. Many of the purchases have been luxury automobiles and four-wheel-drive vehicles that have saturated the Colombian automobile market.”
In 1991, a New York Times article noted that drug trafficking in Colombia was contributing to deindustrialisation and, therefore, unemployment in the manufacturing sector:
A big problem is that the drug profits are repatriated as contraband goods. Colombia’s two largest cities, Bogota and Medellin, have large shopping centers, both called San Andresito after Colombia’s San Andres Island in the Caribbean. Most contraband passes from the island to these bulging inland malls. Contraband sales are estimated at $1 billion a year. But the large contraband trade has contributed to the country’s “disindustrialization,” a study by the Bogota economic research group Fedesarrollo, has found. Local industries compete with the goods and are consequently forced out of business. And the drug barons walk away with local currency to spend on luxuries: fleets of sports cars and motorcycles, exotic animals and art works. Since most of those goods are imported, there is no expansionary effect on the Colombian economy.
Today, the estimates of the value of illicit financial flows related to drug trafficking in the western hemisphere are between $80 – $90 billion a year; enough, that is, to have an impact on currency values or influence macroeconomic policy.[4] One of the obstacles to combatting these illicit financial flows is that traffickers now take advantage of the same mechanisms used by the very wealthy and corporations, including tax havens. To crack down on laundering of illicit gains would mean addressing the loopholes in the legal system which allow for financial secrecy. A drug trafficker, for example, will launder money using the same means as a corporation sending bribes to government officials. As one study observes, while officials have constantly promised reform, “We have waited long enough now to conclude that they are insincere.” The American justice system in particular demonstrates “a curious indifference to white-collar crime.”
Another UNODC study has discussed the way drug trafficking – through its macroeconomic effects and, citing the DEA, “short-run positive effects” – can influence policy decisions:
[T]he political dilemmas posed by the illicit drug industry are not limited to personal enrichment. For some Governments, even with the best of intentions, worsening terms of trade mean that hard currency revenue – drug-tainted or not – have special appeal even at the official level. For those faced with seemingly untenable debt-servicing burdens, drug money can be seen as a panacea for a vast array of other public commitments. In 1992, the proportion of external debt to GNP was 84 per cent for Bolivia, 48 per cent for Pakistan, 95 per cent for Peru and 386 per cent for Zambia. In such desperate situations, officials find themselves caught in a dilemma between looking the other way in order to finance governmental expenditures and enforcing laws against drug trafficking. In financial markets, Governments often find themselves in an analogous situation: by relaxing controls and establishing safe-money havens in order to woo investors, they run the risk of attracting illicit funds, losing creditworthiness and lowering prospects for long-term financial stability.
Drug trafficking, therefore, may lead to circumstances that condition the kinds of macroeconomic policies that are pursued. And there may be other ways in which economic reforms benefit local groups reliant on illicit incomes. The obvious example is Afghanistan. Soon after the occupation, the country adopted – or, more correctly, the occupying forces and the international financial institutions imposed – an economic model based on the “Washington Consensus” reforms.[5] A long-recognised effect of a free trade regime in a poor country is that it will hold in place the existing production structure: a country that exports rugs and grapes, and adopts free trade, will most likely be exporting the same kinds of products ten years later. The economic model, noted a World Bank report, had led to a “market-oriented overall policy environment, few legal constraints on labour markets, and a generally untrammelled informal sector.” Commenting on the beneficiaries of such a model, Erik Reinert, an economic historian and development economist, writes: “Warlords in the world periphery may appreciate free trade [because it] locks a nation in a pre-capitalist and backward economic structure that prevents democracy.”
The privatisations and the economic liberalisation that followed the occupation of Afghanistan were, it seems, a great boon to the political and business elite involved in the drug trade. There are other dynamics to be considered. In Colombia, for example, the paramilitary forces are financed by the drug trade. These groups have historically been the shock-troops of the government’s economic model. By assassinating trade unionists, they contributed to the extremely low rates of union membership and stifled calls for changes in the economic model. The murder of progressive politicians, by paramilitaries and traffickers, had a similar effect. Land grabs by paramilitaries also helped consolidate land ownership and the model of development based in large part on oil, mining and monoculture; studies have even shown that “violence perpetrated by armed groups sympathetic to the interests of the oil sector – namely, the public armed forces and right-wing paramilitaries – have facilitated FDI in Colombia’s oil sector.” We therefore have a self-reinforcing system: an economic model beneficial to criminal groups, combined with violence funded by illicit income that serves to perpetuate that model. A coalition of NGOs in Colombia have referred to the national economic model as “pro-rich.” For a number of reasons outlined here, it may also be “pro-criminal.”
In my report, I discussed another neglected area: the relationship between economic reforms, deindustrialisation and criminal gangs. Throughout Latin America, economic liberalisation has led to the decline of manufacturing industries that were a source of relatively well-paid jobs. Medellin, for example, was once an important textile centre. When the industry disappeared, young people were left with few viable options for employment. Criminal gangs offered an alternative. Similar phenomena are observed across urban areas of Latin America. And the same issues exist in the countryside: it is in the interest of the traffickers and their facilitators to have a large proportion of farmers rely on an illicit cash crop in order to survive.
Identifying the sources of such problems guides us towards possible solutions. As I write in the policy brief:
“From the perspective of a development economist, the fact that in Guatemala City thousands of young men decide to join local gangs cannot be separated from a production structure which revolves around exports of bananas, coffee and sugar. In Colombia, the key to the perennially high levels of coca cultivation is the government’s exclusionary economic model focused on extractive industries, monoculture and finance, which cannot absorb the labour abandoning the countryside and leaves around half the working population in the informal economy. If Afghanistan continues to focus on exporting carpets, rugs and dried fruits, its farmers will never have any other option than to produce illicit crops to survive.”
[1] A related issue is the liberalization of capital accounts, a policy that has been embraced by a number of developing countries. These measures increase the economic vulnerability of a country, and go far beyond the original recommendations of the so-called ‘Washington Consensus’. Allowing the free flow of capital out of the country grants investors the power to ‘discipline’ governments who make economic policy decisions to which they are opposed. It will also facilitate money laundering. As one study notes, capital account liberalization should not take place until the government has made sufficient strides against “corruption, crime, illegal businesses and money laundering.” This was clearly not the case in countries like Colombia or Brazil. http://www.unece.org/fileadmin/DAM//ead/ptepf/daianu_ptepf_28_06.pdf
[2] In Colombia, foreign currency, primarily dollars, flooded the black market. And this caused an inversion of the normal arrangement: buying pesos on the black market was more expensive than the official rate. This suggests a surplus of foreign currency, and a willingness of traffickers to pay a premium to convert their currencies, without uncomfortable questions being asked.
[3] And, it should be remembered, what harms agriculture is beneficial to those who need farmers to rely on illicit sources of income to survive.
[4] One of the results of the pandemic has been a worldwide increase in cash holdings. Part of this development could be attributed to less retail activity, meaning criminal groups have been unable to launder their money, and are forced to hold cash. See here for discussion.
[5] For an excellent analysis, see: Del Castillo, G. Guilty Party: The International Community in Afghanistan, Xlibris Corporation, 2014
The 2020 United States presidential election—with early voting underway and Election Day on November 3—is already like no other in history. In a pivotal year the presidential campaign has been repeatedly shaken by seismic events: a devastating pandemic, George Floyd’s killing by police officers, and subsequent protests, President Donald Trump contracting COVID-19, and Trump himself claiming that the vote will be fraudulent.
With the election likely being decided on the merits of each candidate’s “character” an analysis of their positions on drug policy is a fascinating measure. With so many other high-profile issues competing for attention – COVID-19, the economy, Supreme Court nominations – drug policy will not be a deciding factor in the 2020 election. Indeed, it seldom is in any Presidential contest. However, the influence of the winner on Health Care and Criminal Justice systems will directly affect the nation’s drugs policy and an analysis of the candidates’ evolving positions on the issues reveals some important differences between the candidates.
‘How it started. How it’s going’ is a trend currently sweeping Twitter and sees Twitter users sharing experiences about their lives, careers and relationships. If we look at the stances of Trump and Biden on drug policy in the same context we see fascinating diametrically opposite movements. Joe Biden – often considered to have been one of the main “architects” of the 1980 and 1990 “War on Drugs,” now has a far more liberal attitude towards U.S. drug problems while Donald Trump’s track-record during office offers little hope for radical changes in the status quo.
Background
Before COVID-19, the U.S. was already battling an overdose crisis of unprecedented proportions, caused by prescription analgesics and illicitly manufactured fentanyls, heroin, cocaine, methamphetamine (alone or in combination). The Centres for Disease Control reports that from 1999 to 2018, over 750,000 people died from a drug overdose with the number increasing each year. Then in 2018 Trump claimed credit for the first drop in 25 years, a decrease of 5% in 2017-2018. Deaths totalled 68,557 – the dip mainly due to a reduction in deaths from prescription opioid painkillers. But it didn’t mark a true turning point in the trajectory of this crisis; the next year 70,000 people died of drug overdoses and 72,000 in 2019, a record high. Provisional data indicate that drug overdose deaths will increase again in 2020, a situation further complicated by the pandemic.
Other issues that had previously dominated the domestic drug policy landscape, such as cannabis legalization, have been eclipsed by recent developments and more pressing issues. Once a ‘third-rail issue’, views have changed in Washington, mainly due to the wider acceptance of cannabis use across the population. More Americans now support the legalization of marijuana, whether for recreational or medicinal purposes, than oppose it. A 2019 Gallup poll indicated that Democrats and Independents overwhelmingly supported legalization and even the majority of Republican voters were for it – albeit by much close margins. The MORE Act (Marijuana Opportunity Reinvestment and Expungement Act) was expected to have been passed by the House in late September 2020. It would have removed federal penalties for marijuana related crimes by deleting cannabis from the Controlled Substances Act and erase some criminal records. However, the motion was delayed until after the election (so that the House could concentrate on coronavirus relief legislation).
So where do the developments in the United States sit within the global drug policy debate? The United Nations Commission on Narcotic Drugs (CND) has also decided to delay until December 2020 a vote on the potential global rescheduling of cannabis for medical purposes, recommended by the World Health Organization (WHO). James Walsh, leader of the US delegation to the CND expressed regret at the U.N. delay, but he also noted that the US delegation’s concern is on what it considers more pressing drug control issues such as “continue to combat the global opioid crisis and synthetic drug threat”.
Trump’s record on drugs
Back in 1990 at a luncheon held by the Miami Herald, Trump called the United States’ drug enforcement policy a ‘joke’ and was quoted as saying “We’re losing badly the war on drugs. You have to legalize drugs to win that war. You have to take the profit away from these drug czars.” He advocated using tax revenues from legalized drug trade to educate the public on the dangers of drugs. However as a candidate for the White House in 2016 he did a 180-degree flip, saying cannabis regulation was “bad” and that decisions should be left to each state to decide its marijuana policy. One of his first appointments as President was to bring in Jeff Sessions as Attorney General, one of many in Trump’s administration who have openly opposed pro-marijuana legislation. In a leaked recording from 2018, Trump was heard to say marijuana makes people “lose IQ points” and at an opioid summit that same year at the White House, Trump advocated the death penalty for drug dealers, equating the provision of lethal drugs with murder. He was quoted as saying “Some countries have a very, very tough penalty — the ultimate penalty — and by the way, they have much less of a drug problem than we do”.
The Trump administration’s lack of focus and failure to act decisively in response to the nation’s drug crisis have frustrated progress over the last 4 years. In 2019 government auditors reported that the Office of National Drug Control Policy (ONDCP), tasked with leading efforts to tackle illegal drug use, has not delivered on a central mission, which was to produce an annual strategy to guide federal agencies and to allocate billions of federal dollars. The ONDCP failed to produce reports in 2017 or 2018 and the first report produced in 2019 lacked the necessary depth and analysis required to be effective – it was only 23 pages long. In February 2020 just prior to the widening COVID-19 pandemic the office published its 2020 Drug Control Strategy. Despite claiming that “The President’s top priority remains, as he articulated in his first strategy, to address, head on, the current opioid crisis and reduce the number of Americans dying from these dangerous drugs”, the document lacked useful information and planning and failed to provide detailed metrics and objectives, as it was legally required to do.
The ONDCP claims achievements in expanding availability of the overdose reversal medication, naloxone; increasing anti-opioid misuse education campaigns for young people; and securing historic funding levels for anti-trafficking efforts and addiction recovery. However data from ambulance teams, hospitals and police shows the number of suspected overdoses has jumped nationally during the pandemic (18 percent in March, 29 percent in April and 42 percent in May), and ONDCP has be woefully slow in responding.
In June 2020 the ONDCP launched the Rural Community Tool Box which is aimed at helping patients access treatment remotely. The Trump administration has designated $425 million in emergency funding for mental health and substance use treatment, but critics say it is not nearly enough to keep afloat treatment programs, recovery centres and needle-exchange programmes. Social isolation, economic hardship and new suppliers and substances have compounded the threats to drug users during the pandemic. So far, the Trump administration has made little real progress in addressing these pressing issues and shows little sign of doing so in the future. The Trump 2020 website doesn’t include any campaign promises. There is some mention of the opioid crisis on the ‘Promises Kept’ section but no indication of the direction of any future drugs policy– or any policies for that matter. We can only deduct from this that his position remains relatively unchanged.
During his first Presidential Campaign much of Trump’s drug policy proposals revolved around the building of “a wall” on the U.S.-Mexican border to stem the flow of drugs and drug dealers. Although he has partially delivered on this campaign promise the pandemic has shown that closing the border with its southern neighbour will not solve the U.S.’s drug problem. During the pandemic the drug flows have been interrupted along with legal commerce but America’s drug problem has not abated and dealers and users have found other, home-produced substances, often with deadly consequences.
In June 2020, following weeks of often violent protests following the death of George Floyd, Trump declared “I am your president of law and order,” emphasising this by tweeting “LAW AND ORDER” in block capitals. This latest mantra doesn’t speak directly to drug policy, since like many of Trumps outburst it doesn’t refer to any particular policy or strategy, but it may include a renewed emphasis on harsher drug related penalties. Evoking fear of “crime” in the electorate has been a feature of American political strategy for years, and was a key feature of Trump’s 2016 campaign, in which Trump vilified immigrants as violent criminals. However, recent polls have indicated “violent crime” is not a top issue for voters, ranking fifth in importance behind the economy, healthcare, supreme court appointments and the coronavirus.
On October 3rd in a proclamation on National Substance Abuse Prevention Month, 2020, the President assured the nation that “we renew our unyielding commitment to breaking the grip of alcohol and drug addiction.” He acknowledged “Addiction to alcohol, illicit drugs, and prescription medications fuels havoc, heartache, and hopelessness in the lives of far too many Americans, as well as their friends and family members.” This seemingly sympathetic concern came only days after the first, disordered, presidential debate in which he mocked Joe Biden’s son, Hunter Biden’s, history of drug addiction.
Biden’s record on drugs
Joe Biden’s record as a U.S. Senator since the 1970’s, including periods as Chair of Senate Committee on the Judiciary (1987-1995) and Chair of the International Narcotics Control Caucus (2007-2009)—as well as his service as 47th Vice President of the United States (2009-2017)—affords a substantial amount of evidence about his stance on drugs policy. However, as with Trump, it is not straightforward. Like Trump, Biden’s beliefs started a long way from where they appear to be now.
Image by: Gage Skidmore from Peoria, AZ, United States of America
During his early years in the Senate, Biden was instrumental in some of the most significant crime bills in recent U.S. history. The Comprehensive Crime Control Act of 1984 established mandatory minimum sentences for drug offenses; the 1986 Anti-Drug Abuse Act, introduced much harsher sentences for possession of crack than for powder cocaine; and the Anti-Drug Abuse Act of 1988, again stiffened prison sentences for drug possession, enhanced penalties for transporting drugs, and established the ONDCP. In 1989, Senator Biden went on national television to criticize President George H.W. Bush’s plan to escalate the War on Drugs, saying it didn’t go far enough; “Quite frankly, the president’s plan is not tough enough, bold enough, or imaginative enough to meet the crisis at hand”. He called for harsher punishments for drug dealers and to “hold every drug user accountable”. In the address he also called for greater spending on drug awareness education, to “do more, and now”.
By the early 1990s, as violent drug related crime continued to rise, in a speech on the Senate floor, Biden wanted to “Lock the S.O.B.s up.” In 1994 Biden boasted, “The truth is every major crime bill since 1976 that’s come out of this Congress, every minor crime bill, has had the name of the Democratic senator from the State of Delaware: Joe Biden [on it]”. The Violent Crime Control and Law Enforcement Act of 1994, the largest crime bill in U.S. history, was also known as the Biden Crime Law. The laws Biden helped shape in the 1980s and 1990s, and similar legislation in states across the nation, marked a trend towards stricter sentencing laws for drugs and violent offenses, resulting in mass incarceration that overwhelmed America’s black communities.
This is not lost on the Trump 2020 campaign. A video ad reminded (Black) voters “Joe Biden’s policies destroyed millions of black lives” and a tweet by @AmericaFirstPAC claimed “Biden was the chief architect of mass incarceration and the War on Drugs”.
Biden’s positioning has often reflected the politics of the time. Democrats and Republicans have battled to prove that they are the toughest on crime. However as the numbers using illicit drugs keep rising and the collateral consequences of disproportionately incarcerating poor people of colour is still devastating lives, Biden has done a volte-face on his ’80s and ’90s stance. The Obama administration, faced with a growing opioids crisis, worked to reshape how America approached the drug problem by pushing for public health response rather than the “tough on crime” approach taken by previous administrations dealing with drug epidemics; heroin (Nixon, 1960s) and crack cocaine (Reagan, Bush, Clinton, 1980s & 90s). Biden backtracked on tougher prison sentences for crack cocaine that he had shaped and he’s acknowledged his previous ‘mistakes’, saying in 2008 “I am part of the problem that I have been trying to solve since then,…because I think the [crack-powder] disparity is way out of line.” During his 2020 run for office he has admitted “I haven’t always been right,” and speaking to criminal justice issues he acknowledged that, “I know we haven’t always gotten things right, but I’ve always tried.” A point he reiterated in the final presidential debate on 22 Oct 2020, repeating that previous laws had been a “mistake” and stating, “No one should be going to jail because they have a drug problem.” Biden’s 2020 campaign website states if elected he will “Reform the criminal justice system so that no one is incarcerated for drug use alone” and “Decriminalize the use of cannabis and automatically expunge all prior cannabis use convictions”, although he does still appear to fall-short of backing full legalization.
Biden’s choice of running-mate, Kamala Harris, has had a similar rethink on her position. The former Californian Attorney General who has a history of aggressive prosecution of marijuana cases is now a vocal supporter of reform. In 2018, she co-sponsored Sen. Cory Booker’s Marijuana Justice Act that would remove cannabis from the Controlled Substances Act and expunge existing cannabis-related criminal records, and was the MORE Act’s lead Senate sponsor. In the Vice Presidential debate on October 8, 2020, Harris vowed that marijuana would be decriminalized at a federal level in the United States under a Biden administration, a move that saw the shares of U.S.-listed major cannabis producers surge the following day. Harris’ stance in fact goes even further and she now appears to support full legalization. In her book, The Truths We Tell (2019) she writes “We need to legalize marijuana and regulate it. And we need to expunge nonviolent marijuana-related offenses from the records of the millions of people who have been arrested and incarcerated so they can get on with their lives.”
Biden’s change of heart may also be down to his own personal experiences. In 1999, his daughter Ashley was arrested in New Orleans for possession of marijuana while attending Tulane University but was not prosecuted, while his son Hunter has had a well-documented drug problem. In that first, already infamous presidential debate, he was provoked by Trump on Hunter Biden’s troubled history he responded “My son, like a lot of people, like lot of people you know at home, had a drug problem. He’s fixed it, he’s worked on it. And I’m proud of him. I’m proud of my son.” With so many American lives touched by the devastating consequences of illicit drug use this message of compassion and care, in the face of stigmatization and scorn, and Biden’s about-face turn may play well with American voters on November 3rd.
Already amidst an overdose crisis of historic magnitude Trump’s administration over the past 4 years has failed to make any significant steps to address the issue and shows little appetite to take the lead on cannabis policy reform. The COVID -19 crisis has only served to highlight failures in a fundamentally broken system, on top of which future U.S. drug policy will have to deal with the legacy effects of the pandemic. While both candidates have over the years shown significant reversals on drug issues, the Trump campaign does not signal and appetite for any specific, further change of direction if re-elected. While a future with Joe Biden as President may offer a more progressive approach to drug policy the repercussions of the events of 2020 may make substantial change more challenging and protracted.
By John Walsh, Tom Blickman, Martin Jelsma and Dave Bewley-Taylor
This Op-Ed was originally published in iPolitics on December 11th, 2017
Buzzing in the background of Canada’s debate on cannabis legalization is the issue of the three UN drug control treaties, and what to do with them.
The issue arose during the House of Commons’ consideration of Bill C-45, and may well come up again now that the bill is coming under Senate scrutiny. There is no doubt that legalizing and regulating cannabis markets for non-medical use will mean Canada is no longer in compliance with the obligation under the treaties to restrict cannabis to “medical and scientific” purposes. And Canada will need to address those treaties — in due time.
However, what ‘due time’ should mean has been the subject of some alarmist commentaries. It has been argued that Canada should have initiated the process of withdrawing from the treaties by this past July 1 to avoid a breach of international law when cannabis is legal for recreational use in July, 2018, as the government intends. Some have suggested that, by missing this supposed deadline, Canada has now limited its legal options and might even suffer international sanctions if its reforms continue as scheduled.
This raises two key questions. Did the supposed July 1 deadline really exist? And does Canada really now have fewer options with regard to managing the mismatch between cannabis regulation and UN drug treaties?
The 1961 UN Single Convention specifies that if formal notification of withdrawal from the treaty is submitted before July 1, it takes effect on January 1 of the next year; if notification is submitted after July 1, then withdrawal takes effect a full year later. But at this stage in Canada’s reform effort, the mechanics of the treaty withdrawal process do not dictate hard deadlines. The alarmism about treaty violations, deadlines and delays is misplaced.
Canada certainly has important decisions to make about how to ensure that its impending cannabis reforms will align with its international obligations. As we describe in our report Cannabis Regulation and the UN Drug Treaties: Strategies for Reform, a range of alternatives merit Canada’s careful consideration. Beyond simply withdrawing from the drug treaties, these options include the possibility of withdrawing from and then rejoining the treaties with reservations (a procedure that Bolivia used with regard to coca) or of modifying certain treaty provisions by means of a special agreement among a group of like-minded countries.
In reviewing its options, Ottawa would be wise to be protective of Canada’s positive reputation as a country that upholds international law. But there is no need to postpone the regulation of cannabis, and there is also no reason to rush to withdraw from the drug treaties — certainly not before the relevant legislation has even become law, and not even immediately afterwards.
The experience in Uruguay — the first country in the world to regulate cannabis — demonstrates why immediate withdrawal from the treaties is not necessary. Having justified its policy position via its human rights obligations, Uruguay has suffered no negative consequences beyond mentions in the annual reports of the International Narcotics Control Board (INCB), the watchdog of the UN drug conventions — noting that the country’s law regulating cannabis is contrary to the provisions of the drug conventions and urging a resolution.
The United States — where eight states have legalized adult-use cannabis and where the federal government has adopted a policy of accommodation — has received a similar message from the INCB regarding Washington’s legally dubious interpretation of the drug treaties.
Canada has better and more legally-grounded options, and plenty of time to consider them carefully. A good starting point would be for Canada to publicly acknowledge that moving forward with regulation of adult-use of cannabis will result in a period of respectful non-compliance with certain treaty obligations — a route that, in the absence of a seamless transition, displays the appropriate regard for international law.
Canada could explain the reasoning behind its reforms and why the country’s new regulatory approach is justified by the need to realize other domestic and international legal and policy commitments, particularly with regard to public health, child protection and human rights.
Canada is not alone in reforming its cannabis policy, nor is it the first. In addition to Uruguay and the eight U.S. states, many local authorities in other countries, notably in Europe, are pushing national governments to follow suit. In the Netherlands this has resulted in the October 2017 decision of the new coalition government to allow for experiments with regulated supply of cannabis to coffee shops. This would extend toleration of cannabis sales in these premises to tolerated regulation of the supply.
Meanwhile, the World Health Organization has initiated a review of the classification of cannabis under the drug conventions. Canada’s cannabis regulation is part of a bigger trend and there is no reason to rush to unilaterally withdraw from the drug conventions. Acting unilaterally may not even be in Canada’s best interests; it could be wiser to act in concert with like-minded states.
The bottom line is that Canada ultimately will need to choose a path forward with regard to cannabis regulation and the drug treaties. But there is no need for hasty decisions and plenty of time for Canada to evaluate its options — and act when the time is ripe.
This blog shows the intimate ties between the international and domestic domains of drug control. This is a well-known phenomenon; however, it involves considerable complexity. The lengths to which governments will go to reduce potential tension at the international level are apparent. This is especially so when states – as in the following case – are wary of the US position. At the same time, powerful domestic forces can counteract the influence of international powers, even when the United States is concerned, as in the aftermath of the Second World War.
The blog selects the example of Britain during that period in which the negotiations leading to the Single Convention were taking place. The then-famous ‘British System’ of drug treatment was a key aspect of Britain’s drug policy relationships; stemming from Sir Humphrey Rolleston’s inquiry into addiction that reported in 1926, the ‘British System’ permitted any doctor to supplyheroin, morphine, cocaine and other drugs to those who were dependent upon them. Unlike the present mode of ‘Heroin Assisted Treatment (HAT), the British System imposed few requirements on patients, who could take their prescription to a pharmacy, collect their drugs and consume them more or less at will. This depended on the regulatory context, the liberal views and the largesse of the doctor, but these were generally forthcoming.
Both the international and the domestic domains played a part in the changes that overtook the British regulatory framework in the 1950s and 60s, leading to the demise of the ‘British system’ of prescribing and its replacement with a much more restrictive ‘clinic’ system in 1968. The international dimension was always important, but in the period preceding the agreement of the 1961 Single Convention, it was especially significant as countries sought to shape the draft treaty to suit their national interests, or (less rationalistically) to forge the global order of intoxication according to their mythological image.
Sir Humphrey Rolleston
Following the war and the continuing rise of the United States as an international military, political and economic superpower, there was friction between it and Britain over aspects of the latter’s drug policies. The 1955 American attempt to impose a global prohibition on heroin was eventually faced down by the British government after internal pressure from the medical profession in support of the drug’s retention in medical therapeutics, including in the treatment of drug dependence. The medical profession was a powerful force in British politics and culture, sufficient to bring the government to resist US pressure.
Britain’s representative at the Commission on Narcotic Drugs (CND), the policy-making body for the new UN international drug control system, was J.H. ‘Johnnie’ Walker. Bing Spear, the Home Office civil servant who had written extensively on UK drug policy, identified Walker as providing the initiative that led to the first Brain Committee, which, commencing its meetings in 1958, reviewed the British drug control system for the first time since Rolleston did so in the 1920s. Government documentation from the mid- to late-1950s supports this claim. The context for Walker’s views was largely international, with the British System undergoing criticism from a number of countries, particularly the United States, through the mechanism of the new United Nations drug control regime.
In 1955, Walker sent a lengthy and thoughtful memorandum to the Home Office suggesting that it was time to look again at the British drug control system. Despite the system’s smooth domestic running, said Walker: ‘It so happens that a number of problems have arisen, or are on the horizon, which indicate that this is a suitable moment to review the present system of control.’ These problems or potential problems included the proliferation of new synthetic drugs such as pethidine and methadone; the UK policy on addiction (by which was meant in particular the Rolleston-inspired regulations permitting the long term of maintenance of opiate habits and the belief in the ‘stabilised addict’); addict doctors; and improper prescribing and supplies to addicts (the issues surrounding ‘script doctors’). The memorandum paid the greatest attention to the second and the fourth of these categories, replicating the situation that obtained when the Rolleston Committee reported and showing that the issue of doctors prescribing dangerous drugs to addicts had remained at the heart of governmental anxieties. Walker claimed that the Rolleston Committee never intended the ‘lavish supply of dangerous drugs to addicts merely for the maintenance of addiction’. He then made reference to a ‘small but potentially dangerous group of drug addicts (mainly heroin addicts) in London at the present time’. This group was ‘disturbing’, as it represented ‘the first real sign of a significant increase in heroin addiction for very many years’. The group’s members had become addicted young and were mostly under thirty – often nearer twenty; many shared an involvement in one particular field of entertainment and therefore met socially at regular intervals – a reference to the jazz club scene. The social context of this drug use made it ripe for proselytism, contended Walker, ‘always one of the more dangerous features of drug addiction’.
He continued that many ‘appear to obtain supplies from a small number of doctors who make no attempt whatever at cure or even, so far as can be judged, at reduction of the dose. In other words, their addiction is deliberately fed, almost certainly in some instances for purposes of gain.’ Walker concluded that: ‘The “script doctor” who thus makes drugs freely available to addicts represents a special problem…’
Walker’s memorandum showed that the Home Office was by this time fully aware of the flourishing new London addict subculture, a full ten years before these facts were published in the Second Brain Report. As noted by Spear, the peculiar thing is that the first Brain Committee did not address it in their deliberations nor their report. At the Home Office, it was Tom Green (who succeeded Walker at the Drugs Branch) who led the drafting of the advice and information sent to the Ministry of Health, from which emerged the shape of the review. For ‘some inexplicable reason’, while drawing heavily on Walker, Green did not include evidence of the emergence of London’s expanding heroin subculture.
One possible reason for this startling omission lay in the international relations around the topic of drug control. Walker points out that US medical opinion was firmly against maintenance and the notion of the stable addict. The ‘strongly held’ view in the American medical profession was that it is ethically unacceptable to condemn a patient, especially a young patient, to perpetual addiction by offering this form of treatment. It was also remarked that the CND and World Health Organisation were highly critical of ambulatory treatment of the kind practiced in the UK. Indeed at its 10th session, the CND ‘expressed the view that ambulatory treatment (including the so-called “clinic” method) was not advisable and asked the World Health Organization to prepare a study on the appropriate methods of treatment.’ Furthermore, a clause had recently been inserted into the draft Single Convention which spoke of treatment being given on ‘a planned and compulsory basis, in properly conducted and duly authorised institutions’. However, by virtue of a qualifying clause that was initiated by the UK, such measures would be applicable only in those countries having a large addict population; it was this proviso that permitted the UK government to sign the 1961 treaty despite its differences with respect to drug treatment. Notwithstanding this, Walker expressed concern that the general trend at the CND was toward compulsion, and that there may in due course be concerted pressure for the removal of the UK clause. He added that, ‘it is unlikely that the United Kingdom could ever accept an obligation to require compulsory treatment of drug addicts in a closed institution’. In fact, Walker made it clear that such a measure could prevent the UK from signing the treaty, and would have been in conflict with the overall trend of mental health policies in Britain at this time, as expressed in Lord Percy’s 1957 Report of the Royal Commission on the Law relating to Mental Illness and Mental Deficiency. This optimistic document led the trend away from confinement, toward voluntary and community based mental health treatment, and fed into the 1959 Mental Health Act. In relation to addiction, Walker commented in closing that: ‘There is a limit to what the State should attempt, and the deprivation of personal liberty for medical reasons is far too serious a matter to contemplate unless there is overwhelming evidence of the need for it because of some widespread and particularly virulent social problem. This need does not exist in the United Kingdom’.
This last sentence is the key one. In order to fight its corner at the CND, the UK government needed powerful evidence that the domestic drug problem continued to be so small as to be negligible, a point which some other countries disputed. Consequently, ‘there would be much to be said from the point of view of strengthening our case in international circles for obtaining an authoritative opinion from a body of experts on the necessity for, and the feasibility of, providing special treatment for drug addicts in this country.’77 In other words, a Committee set up to review Britain’s arrangements could prove very useful in providing the government with ammunition which to fight its international drug policy corner, so long as this evidence indicated that the problem was tiny and relatively insignificant.
Although, as Spear claims, Walker’s superiors at the Home Office were initially unreceptive to his argument, the Brain Committee may well have been influenced by it at the meetings which produced the first report. Green led the way in producing the documentation for the Committee; mention of the expansion of the opiate subculture was entirely absent, and the growth in heroin addiction strongly downplayed. Accordingly, its Report was structured on precisely the lines that would support the government in its negotiations at the CND. It stated baldly: ‘After careful examination of all the data put before us we are of the opinion that in Great Britain the incidence of addiction to dangerous drugs… is still very small.’
This argument remains for the present a speculative one; nonetheless, the omission of the West End heroin subculture from the Home Office memorandum of evidence to the first Brain Committee, and the Report’s conclusion, which supports the UK’s requirements at CND in the run up to the 1961 Single Convention, are highly suggestive. Beyond this specific question, however, it is clear that the construction of international drug policy is a matter of both international and domestic (and transnational) domains, and that it is impossible to understand countries’ conduct in international fora without taking into account international politics and culture. And vice versa.
Dr John Petro
[1] Departmental Committee on Morphine and Heroin Addiction: Report (London: HMSO, 1926). (Rolleston Report)
[2] 59 D. R. Bewley Taylor, The United States and International Drug Control, 1909-1997 (London and New York: Continuum, 1999) p.141.
[3] Spear, H. B. & (ed) Mott, J. Heroin Addiction, Care and Control: The British System. London: Drugscope, 2002. Pp.65-89.
[4] Spear, H.B., Heroin Addiction, Care and Control p.90
[5] The National Archives HO 319/1 and MH 58/565.
[6] McAllister, W. B. Drug Diplomacy in the Twentieth Century: An international history. London and New York: Routledge, 2000. Pp.185- 211.
[7] TNA HO 319/1 ‘Dangerous Drugs Administration and Policy in the United Kingdom’ 25 October 1955.
[8] Ibid.
[9] Ibid.
[10] Ibid.
[11] Ibid.
[12] Ibid.
[13] Spear, H.B., Heroin Addiction, Care and Control, p.92.
[14] Ibid.
[15] The Tenth Session of the Commission on Narcotic Drugs, 1955. http://www.unodc.org/unodc/en/data-and-analysis/bulletin/bulletin_1955-01-01_2_page005.html Accessed 3rd September 2016
[16] TNA HO 319/1, ‘Dangerous Drugs Administration and Policy in the United Kingdom’ 25 October 1955. In this passage, Walker was quoting from a 1954 CND draft of the Single Convention.
[17] Ibid.
[18] E. Percy Baron of Newcastle Report of the Royal Commission on the Law relating to Mental Illness and Mental Deficiency (London: HMSO, 1957).
[19] TNA HO 319/1, ‘Dangerous Drugs Administration and Policy in the United Kingdom’ 25 October 1955.
[] Report of the Interdepartmental Committee on Drug Addiction 1961 London: HMSO. Paragraph 24.
After countless reforms and billions of investment eradicating coca cultivation is still a great challenge for Colombia.
Ross Eventon, GDPO
Early March, 2017: The United States government and the United Nations announce large increases in the amount of coca being cultivated in Colombia.
The head of the US Bureau of International Narcotics and Law Enforcement Affairs flies to Colombia and meets the President. The increase is due to the end of aerial fumigation operations, he says, but he also assures the press that he would not be asking the government to restart that policy….
Continue reading full open access article here: http://www.aljazeera.com/indepth/opinion/2017/04/coca-production-rise-colombia-170419130227958.html
The Maghreb countries, part of the Arab Maghreb Union, are Algeria, Libya, Mauritania, Morocco and Tunisia and form the largest part of North Africa. These countries are currently in the centre of the boiling issues of the world including terrorism, human trafficking and drug trafficking. These countries are large consumers and producers of plant-based and synthetic l psychotropic substances, Morocco being the largest cannabis producer in the world in 2014. But when it comes to discussing the issue of drug use, the legal response to it, and its impact on society, the debate focuses on ideological issues of morality and the rejection of illicit drugs, as data on the prevalence of drug use and the patterns of the use in these countries are missing.
The Maghreb is also part of the MENA region (Middle East and North Africa), which is one of the two regions in the world in which new HIV infections are increasing (with Eastern Europe and Central Asia) and largely driven by drug injection. In 2014, the region has seen HIV infections related to drug injection represent 28% of all new infections, and this represents a minimum since it is based only on often incomplete data submitted by governments. The region is also home to an estimated 630,000 people who inject drugs. This blog will analyze the current situation in two major countries of the region, Algeria and Morocco, which have chosen different approaches to drugs, and compare the outcomes of their policy choices. The blog will finally highlight the current drug policy reform discussions in both countries.
The current official drug prevalence:
Morocco is the country with the most widely available data in the region, with an estimated injecting population of 3000 to 4000 according to the Ministry of Health. Drug injection is concentrated in the North and East of the country, in the transit regions that export cannabis to Algeria and Spain, and import amphetamines (mainly from Algeria) and heroin (mainly from Spain). The country is also the first Arab country, and the second in Africa, to have introduced methadone substitution therapy in six centers in 2011. Furthermore, it is among the two only countries that have a national harm reduction policy in the Arab world, the other being Lebanon. The prevalence of HIV in the general population is of 0.14% (0.1%-0.2%), and mainly concentrated among key affected populations, with people who inject drugs (PWID) representing 10.17% of this total. The country has introduced methadone therapy in prisons as a pilot project , but the author has been informed that the experiment will be extended to five penitentiary centers throughout the country in the coming months.
In Algeria, the situation of PWID or people who use drugs without injection is undocumented. There is no official data on the prevalence of drug use in the country, but it is known that cannabis is the most widely used substance in the country and its use has doubled in the course of two years, between 2012 and 2014. PWID living with HIV represents 1.1% of those tested in 2014, for a prevalence rate among the general population of less than 0.1%. In 2014, a study by the National Office on Drugs and Addiction (Office national de lutte contre la drogue et la toxicomanie) showed that the number of people who use drugs (PWUD) is 250.000, while simultaneously independent research by the FOREM (Fondation nationale pour la promotion de la santé et le développement de la recherché), a non-governmental organization, estimated PWUD to be one million people in the country. A 2006 study on the number of PWID in developing countries reveals that Algeria is the second highest burden country in all North Africa following Egypt, with a number of PWID reaching 40,961.
The two neighboring countries, the largest demographically in the region, hegemons politically and dynamic economically, are at odds largely due to their conflict on the Western Sahara, Morocco claiming its territorial integrity includes the said territory, while Algeria hosts and supports, diplomatically and financially, the separatists. The conflicting relationship between the two countries is also represented in the cooperation against drug trafficking, where they accuse each other of knowingly enriching their respective black markets of illicit drugs. Publicly and through official press conferences, Algeria accuses Morocco of the impact of the large amounts of cannabis being smuggled by the Rif traffickers, while Morocco reminds Algeria that it is one of the largest producers of psychotropic substances that flood the Moroccan black market.
The narcotic laws and drug use:
The laws in Algeria and Morocco punishing drug use and possession are harsh, as they are in the rest of the African and MENA regions. The Algerian law (Law No. 04-18 of 25 December 2004) imposes incarceration between two months to two years in addition to a fine from five to fifty thousand Dinars (fifty to five hundred US dollars) or one of the two sentences for personal use or possession. For a similar offence, a Moroccan convict will face imprisonment of between two months and one year in addition to a fine (Dahir No. 1-73-282 of 21 May 1974), or one of the two sentences. Meanwhile, the Moroccan law remains the least harsh policy in the region. In 2014, 31% of the cases treated by tribunals in the country were related to illicit drugs.
The Algerian narcotics law differs highly from its Moroccan counterpart since it gives precedence to prevention over punishment, as it states preventive and treatment measures before penal judgments. It makes treatment the basis of the legal response to drug use, and sanctions are not enforced if and until the treatment is refused. In addition, returning to treatment when necessary is not prevented even in cases where the treatment decision was previously refused (Article 9 of the law). Sanctions on drug consumption have been reduced for the following reasons: First, punishment for possession or consumption would be imprisonment of between two months and two years. This is a lighter sentence than lockup or hard labor and indicates that drug consumption or possession for personal consumption is considered a misdemeanor rather than a felony; second, the law authorizes the judge to choose between imprisonment and a fine and does not force him to combine the two and third, the judge’s authority to determine the sanction provides some autonomy as to whether imprisonment or a fine is chosen, as there are large differences between the minimum and the maximum limits.
These parameters of the law, that are presented as a prioritization of public health over punishment in drug policy, are still problematic as they allow for the institutionalization of mandatory treatment. According to Article 7 of the law, the examining magistrate or juvenile judge may order detoxification, accompanied by medical surveillance and rehabilitation for “any drug user whose condition requires these measures”. The court’s judicial authority, in this case the specialized judicial authority, may also rule exemption from sanctions (Article 8). According to Article 9, incarceration and fines shall only be applied to anyone who refrains from executing the decision to undergo detoxification. The law as it is today gives judges the power to decide on medical conditions and how they should be treated. Despite every effort, it is still difficult to find data on how many people are diverted from tribunals to treatment centers in both countries.
The findings of on-the-ground research:
To face this complex situation, in countries that produce large quantities of illicit drugs, consume heavily and carry the burden of epidemics related to drug injection, non-governmental organizations on the ground have started researching the situation and gathering evidence. The Association de Lutte contre le Sida (ALCS) in Morocco has launched on-the-ground research as early as 1996 in the Northern provinces of the country to map the injection drug use, and respond to the HIV situation. At the time, drug injection has been found to be limited. A 2003 national survey on mental health and addiction, with a sample of 6000 people over 15 years old, has shown that cannabis is the most widely used substance with a prevalence rate of 3.94%, the age of first use was decreasing, and the prevalence of heroin was of 0.02%. In 2006, with the changing nature of drug use and the spread of HIV through drug injection as transmission mode, the Ministry of Health launched situational studies on drug injection, in order to establish the first harm reduction national plan. The first action was to launch needle and syringe programmes, followed by methadone treatment. The harm reduction programme includes several advances, such as the inclusion of civil society in the delivery of services, the dispensing of harm reduction training, and the delivery of services during the night hours. For instance, the ALCS delivers through its mobile unit a needle exchange programme in three cities in the Rif. Nevertheless, the programme faces tremendous challenges, be it within the harsh legal environment or through the obstacles for the scaling up the services delivery.
In Algeria, and as stated earlier, data and monitoring of current drug policies is missing. The Association de Protection Contre le Sida (APCS) has reached out to the Moroccan ALCS to conduct a rapid diagnostic mission to map the drug situation in the capital city Algiers. For this research, 43 PWUD were interviewed, of which 5 were women, 62% were students or unemployed at the time of the qualitative interview, and represented 6 communes of the capital city. The findings concluded that outside of the squats in the Blida neighborhood, drug injection remains a personal activity, that it concerns all ages and all socio-professional categories of society. Regarding PWID, 70% injected Subutex (buprenorphine) and 30% heroin, and poly-consumption was the most shared behavior of the study participants (100%). 33% of those interviewed were incarcerated at some point in their lives, and up to 5 times for some, and for over 25% the imprisonment resulted of a simple possession offence. The study finally has shown that PWID do not access the services they need, since pharmacists refuse to sell them clean syringes, increase substantially their price, or do not have a stock in remote areas. Finally, only the national hospital of Blida offers rehabilitation and abstinence based programmes which are limited in number and do not respond to the needs of PWID.
This first study highlights the situation in Algiers, and is being currently used to advocate for drug policy and harm reduction reform with the Algerian authorities and civil society. In a consultation entitled “the role of civil society in harm reduction” held in Algiers on September 26-27, 2016 attended by the author, the representative of the Office national de lutte contre la drogue et la toxicomanie, the drug control organ under the chairmanship of the Prime Minister, announced that the country will open the first methadone induction service in Algiers in the coming months. No details were given. Moreover, NGOs collaboration between the two countries is in vivid contrast with the non-cooperation of the states on the drugs issue.
Conclusion:
Algeria and Morocco share the same languages (Berber and Arabic), similar colonial historical patterns, and the longest border for both countries. They also share the drug production, use and trafficking since they both produce large amounts of plant-based (Morocco) or manufactured (Algeria) illicit drugs; they share the same trafficking routes from the Sahara or from the Middle East towards Europe; and cannabis is the most used substance in both countries. Nevertheless, the countries have taken different public policies to respond to drugs. Morocco, a traditional and large producer of cannabis, faced with a heroin crisis in the 2000s developed the first harm reduction strategy in North Africa. Algeria, where heroin injection has not been seen as a health crisis until recently, has focused its efforts on the rehabilitation of PWUD.
khalid_blog-maghreb-drug-policy_finalAfter years of designing drug policies, mainly focused on eliminating drugs and curbing the HIV infections among PWID, drug policy reform is becoming a mainstream discussion in Morocco. The political parties PAM and Al Istiqlal have introduced parliamentary bills to legalize the medical and industrial use of cannabiskhalid_blog-maghreb-drug-policy_final. In Algeria, the debate still focuses on the issues related to trafficking and illicit production, and the announcement of a methadone service has been recurrent since 2015 without details on the location or the conditions required to enroll PWID in need of this service.
Following exploratory fieldwork in the rural coca growing fields of Colombia, GDPO followed the cocaine supply chain to Panama. Most recently, time spent on the Northern Caribbean coast soon revealed the permeation of drug trafficking into the already complex socioeconomic context that many perceive as paradise.
Paradise of Bocas del Toro (MandingA 2013)
First impressions of Bocas del Toro – the name of both the 7,000+ person settlement on Isla Colon, just off the north eastern seaboard of Panama, but also the wider surrounding Province – largely confirm its international reputation as an accessible tropical ‘paradise’. With sympathetic afternoon light, the final leg of the 1-hour flight from Panama City reveals aqua marine water lapping at golden sands backed by lush green forests. Once established in the area, other widely talked about attractions of Bocas quickly emerge. There is a wealth of outdoor activities. Many international tourists, largely backpackers, and domestic visitors come to enjoy the Caribbean Sea: to scuba dive and snorkel, surf the notorious waves of Playa Bluff, or to take things a little easier with sunbathing and guided tours to spot the charismatic wildlife.
Party goers in one of Bocas’ bars open late into the morning (Taken by Author 2015)
Another attraction of Bocas del Toro for many, and particularly backpackers, is undoubtedly the opportunity to mix Salsa and Reggaeton music, with low cost national beers and regional rum cocktails, as they enjoy the party life offer on Isla Colon (primarily in BocasTown) and the surround islands. Many of the bars and clubs in Bocas town are right on the water: making it very possible to ‘live the dream’ of enjoying beers in a hammock, dancing off the alcohol, and when things get a little too hot back-flipping off the dock into the cooling sea.
In this hedonistic environment, it is seemingly easy to forget the volumes of boat traffic and not think about the dubious quality of the sea water while enjoying a midnight swim. Another undercurrent in the town is the availability cocaine and cannabis. Sellers freely mix in the nightlife with various degrees of subtly in communicating their offerings. During the day, it is unusual to walk the length of town without being offered ‘weed’ – sometimes as a follow up to the initial list proposal of taking a boat tours to the beach – although there is little menacing about time spent in Bocas, and disinterest is well-accepted by opportunistic sellers.
Part of the reason for the level of supply is the demand of international tourists and more permanent life style migrants willing to pay higher prices than local consumers. However, Bocas del Toro is also well supplied with drugs as one of the recognized points of refuge for traffickers making the journey up the EasternCoast from Colombia to North America
Originally founded as a settlement of concentrated population by foreign banana producers, the region remained disconnected from administration in Panama City due to a lack of a reliable road connection: and therefore, the centralized government administration has lacked a presence in many respects. The archipelago is also composed of some highly remote islands that fall well beyond almost all government services and authority: and as in many cases across the world, the lack of state institutions supports the trafficking of drugs.
View of coastal geography from the air (Author 2015)
Despite limited resources, local law enforcement officers in Bocas confirm that they have been involved in interdiction operations in partnership with central authorities and the US Coast Guard: furthermore, these operations have yielded high powerboats used by the traffickers that are then repurposed for local counter narcotics operations. Discussions with the local police support existing knowledge that traffickers use the inland water ways of the Panamanian coast to evade the authorities during the day, and then make their staged journeys under the cover of night (UNODC 2012). In some cases it is believed that small shipments of drugs are consolidated in Panama before being moved on (UNODC 2012). Local testimony also identified that during chases, traffickers will jettison quantities of drugs in attempts to bribe the police.
It is through a combination of these mechanisms that trafficked drugs enter the Bocas economy. The availability of drugs then provides relatively easy returns for those willing to become involved. This option is especially attractive so some due to the poor quality of education, high levels of poverty and general limitations on livelihood opportunities in the Bocas region. Despite Panama’s average national economic growth of 7.2% between 2001 and 2013, of the mainly indigenous population of the Bocas del Toro province, 25% are classified as poor and 11% as extremely poor (Omar and Moreno 2014). Many of these people live on subsistence agriculture and fishing on outer islands. There is therefore a potentially strong pull incentive to become involved in the distribution of drugs. In this case, as was found in Colombia, rural development will likely be as important an anti-trafficing policy as strengthening governance capacity for interdiction operations.
In conclusion, while the vast majority of visitors to Bocas del Toro find their expectations of fulfilled, the reality is that the international trafficking of drugs is playing into a complex socioeconomic situation, which many of the ‘poor’ permanent residents might well not accept as ‘paradise’. Again, genuine investment in enhancing the life opportunities of those currently motivated to support drugs distribution will likely contribute to a reduction in the global trade in narcotic drugs.
Sources
Omar, A. and V. Moreno ( 2014). Pobreza e Indigencia. Panama, Ministerio de Economia y Finanzas.
UNODC (2012). Cocaine from South America to the United States. Transnational Organized Crime in Central America and the Caribbean A Threat Assessment. Vienna, United Nation Office on Drugs and Crime.
Psychoactive substances or ‘drugs’, often associated with recreational use, are in fact commonly used for a variety of medicinal purposes. It is even less understood that the supply of more than 100 of these drugs is regulated by a complex system of international drug control underpinned by three United Nations treaties with near universal ratification. This post explores the relationship of drugs and international law, specifically international drug control law and international human rights law, using the topical example of placing ketamine under international control.
International drug control law
The legal framework of international drug control is shaped by three treaties: the 1961 Single Convention on Narcotic Drugs (as amended by the 1972 Protocol), the 1971 Convention on Psychotropic Substances, and the 1988 Convention against the Illicit Traffic in Narcotic or Psychotropic Substances. Scheduling is the process established by the treaties to bring certain psychoactive substances under a graded scale of international control. Scheduling a substance creates positive obligations for States to implement regulatory processes that meet or exceed requirements established by the treaties. In some overburdened health systems, this can lead to over-restrictive controls that inhibit medical access to essential drugs, well documented in the case of opioid analgesics.
Uses of ketamine
Ketamine’s unique properties make it one of the most important and widely used drugsin emergency and surgical medicine globally. Where most anaesthetics require electricity for ventilators and gas masks, ketamine—an injectable anaesthetic—can be safely administered in settings without regular access to power, for example, war zones or impoverished rural areas. The analgesic properties of ketamine make its use during emergency surgery, such as for caesarean sections, indispensible for improving mortality outcomes in less-developed countries throughout the Global South. It is because of these properties that the World Health Organisation (WHO) placed ketamine on its list of essential medicines for both children and adults.
Outside of clinical settings, ketamine is used recreationally, although such use is mainly in more developed countries. China, in particular, views the illicit production of ketamine as an “increasingly serious” domestic issue and has repeatedly requested the substance be subject to international control. It is with this direction from China, that ketamine has made its foray onto the international legal stage.
Scheduling ketamine under international law
Established in 1946 by ECOSOC, the Commission on Narcotic Drugs (CND) serves as the principal policy-making body of the UN drug control system and under the three drug control treaties, it is mandated to oversee the scheduling system. China is currently one of 53 members of the CND, and is authorised under the treaties—in the case of ketamine, the 1971 Convention on Psychotropic Substances—to introduce substances of concern for scheduling consideration. Procedurally, article 2 of the 1971 Convention requires the CND to submit scheduling recommendations to the World Health Organisation (WHO) for an evidence-based review to determine if the substance meets the criteria elaborated under article 2(4) to require scheduling (or not) and its degree of restriction under the graded scheduling system. Under article 2(5) of the 1971 Convention, the WHO’s recommendations are “determinative” when it comes to the “medical and scientific” basis for adding substances to a schedule.
This is not the first time China has requested ketamine be scheduled. The WHO’s review this year and each time before (see here and here) determined the public health risks associated with recreational use did not merit any measure of scheduling. The conclusive nature of this recommendation under the 1971 Convention has been subject to much interpretative debate. The current prevailing interpretation has placed the status of such a recommendation within broader considerations such as “economic, social, legal, [and] administrative” factors listed in article 2(5).
What this interpretation signals is that despite WHO’s determinative assessment that ketamine does not meet the criteria for scheduling under article 2(4), its scheduling may now be subject to a purely political process (a two-thirds vote by the CND would place ketamine under international control).
The control of ketamine and international human rights law
The impact the control of ketamine has upon human rights is a critical consideration. While human rights are not explicitly mentioned in the 1971 Convention, they are contained within the meaning of “legal” considerations as written in article 2(5), which States must take into account when deciding to add a substance to a schedule.
As mentioned previously, scheduling a substance creates regulatory barriers that have made essential medicines completely inaccessible for those most in need. These barriers result in on-going violations of human rights—most notably the right to health. The normative scope and content of the right is contained within article 12 of the International Covenant on Economic, Social and Cultural Rights (ICESCR) and imposes upon States core obligations to be given immediate effect. General Comment 14 on the right to health elaborates further that amongst this minimum core is the obligation to provide medicines as indicated on the WHO’s essential medicines list. As such, ensuring ketamine is available, accessible, acceptable, and of sufficient quality forms part of a State’s core right to health obligations.
Should ketamine fall under the scope of international control, any restrictive measures a State subsequently imposes cannot interfere with current levels of access. The imposition of international control requirements would in many States, restrict current levels of access to ketamine and amount to a deliberate retrogressive action in violation of the right to health. This is relevant to any scheduling level under the 1971 Convention. While Schedule 1 imposes the most restrictive control measures, States can apply equally or more restrictive measures for any schedule level under article 23. As such, the same human rights assessment would apply as States with less complex regulatory systems often lump controls into one or two highly restrictive categories—see the example of phenobarbital, a Schedule 4 drug under the 1971 Convention.
As the vote fast approaches, a human rights framework offers States a powerfulnormative counterweight to the political pressure they face to place ketamine—an essential, life-saving medicine—under unnecessary international control.
The Commission on Narcotic Drugs (CND) in Vienna will decide next week between two opposite proposals by China and the WHO about international control ofketamine, an essential anaesthetic in human and veterinary medicine. China originally proposed bringing ketamine under the 1971 Convention’s most severe control regime of Schedule I, which would dramatically affect its availability for surgery in poor rural settings and emergency situations. The WHO Expert Committee reviewed all the evidence and advised against any international control of ketamine, arguing it would trigger a public health disaster.
A fact sheet produced by concerned NGOs, TNI among them, has received endorsements from over 80 organisations around the world, including many medical associations of anaesthesiologists and palliative care. The International Federation of Red Cross and Red Crescent Societies came out with its own statement of concern. At intersessional CND meetings past weeks in Vienna, several countries expressed their worry about the Chinese proposal and questioned the procedural legality of bringing it to a vote, now that the WHO has strongly recommended against it. Confronted with broad opposition, China changed it proposal and now calls for inclusion in Schedule IV instead, the lightest control regime under the 1971 Convention. The move is meant to soothe concerns and apparently several countries that opposed China’s original proposal are considering the softer option as an acceptable compromise.
Adding ketamine to Schedule IV, however, would still negatively impact on its availability in a number of countries, less severely so when compared to Schedule I, but millions of people would still be at risk of not having access to anaesthesia if they require surgery (seeextended fact sheet). Moreover, too little attention has been given in the debate so far to the potential consequences for future scheduling decisions, as this would set a precedent to add substances to the treaty schedules bypassing WHO’s expert advice. In response to questions raised about the procedure, UNODC asked the UN Office of Legal Affairs (OLA) in New York for a legal opinion about the basic question: “Can the Commission on Narcotic Drugs schedule a substance under the Convention on Psychotropic Substances of 1971 if there is a recommendation from the World Health Organization that the substance should not be placed under international control?”. Unfortunately, under time pressure, OLA produced an unhelpful, confusing and questionable legal argumentation concluding that “the Commission can schedule a substance under the Convention on Psychotropic Substances even if there is a recommendation from WHO that the substance should not be placed under international control” (E/CN.7/2015/14).
The 1971 treaty – as explained in detail in its Commentary – established a threshold for substances to be eligible for international control, which requires a careful weighing of their addictive and harmful properties against their medicinal usefulness. The review of the WHO Expert Committee on Drug Dependence is “determinative” regarding medical and scientific matters whether or not a substance meets that threshold. Once the WHO has determined that a substance meets those minimum criteria warranting international control, the CND can discuss the WHO recommendation and consider additional arguments (“economic, social, legal, administrative and other factors it may consider relevant”) to either adopt, reject or deviate from the choice for the particular Schedule recommended by the WHO. As spelled out in the Commentary on the 1971 Convention, if the WHO “recommends in its communication to the Commission that the substance should not be controlled, the Commission would not be authorized to place it under control” (§ 22, p. 71). Clear and simple, it seems, but apparently not for the Office on Legal Affairs.
In its legal opinion, OLA acknowledges that “WHO assessments are determinative as to medical and scientific matters of a substance,” but then continues saying: “but the ultimate authority to decide whether the substance should be added in a Schedule rests with the Commission. In doing so, the Commission is required to take into account factors broader than medical and scientific factors.” The CND “is expected to take a broader perspective, and is required to take into account all relevant factors to reach a conclusion.” On those grounds OLA then reaches its controversial conclusion quoted above, contradicting the official Commentary, and clearing the path – though the OLA advice is not binding in any way – for bringing China’s proposal for scheduling to a CND vote next week. Two-thirds of the 53 CND Member States would need to vote in favour to adopt it, in other words if 18 countries vote against it or abstain from voting the proposal would be rejected.
Following OLA’s treaty interpretation means that the other factors that the CND needs to consider (economic, social, legal, administrative) may provide sufficient reason for adding a substance to a treaty schedule, including if the substance does not meet the required threshold of dependence-producing and harmful properties. The OLA opinion confuses the clear intention of the treaty to establish a minimum threshold to be determined on the basis of medical/scientific evidence by the WHO, with the subsequent discretion of the CND to deviate from WHO’s specific recommendation about which schedule would be most appropriate, after taking into consideration other factors. It is difficult to understand how OLA arrived at such a fundamentally flawed judgement.
OLA also looked into the scheduling history to determine whether there have been any precedents for the situation the CND is confronted with now in the case of ketamine. Two previous cases, in 1991 and 1999, were identified as possibly relevant cases to consider. After acknowledging their different nature compared to the question at hand and that “these two cases seem to indicate that the Commission has generally followed WHO recommendations”, OLA then concludes in what again appears to be a difficult-to-follow twist of the argument that “the practice of the Commission to reject WHO recommendations is still relevant as it indicates that the Commission has not felt itself bound by WHO recommendations.” For the matter under consideration not only a confusing but also an irrelevant remark, because nobody questions that the CND has considerable discretion under the 1971 Convention (more than allowed under the 1961 Convention) to deviate from WHO scheduling recommendations. The treaty and the Commentary make very clear that indeed, the CND is not “bound by WHO recommendations”. The one thing the CND is not allowed to do, however, is scheduling a substance that the WHO has reviewed and concluded that it does not meet the threshold that warrants international control. In the case of ketamine, the WHO has reviewed and decided that three times now…
In one of the previous cases the OLA refers to, arguments were raised in the procedure that could in fact be relevant for the current situation. In short, Spain, worried over the amount of new psychoactive substances appearing on the market, tabled in 1999 a proposal to add all isomers, esters and ethers of substances already on Schedule I or II, placing all such chemically similar substances under the same control. The WHO reviewed the Spanish proposal, and recommended instead to only add substances falling under the much narrower definition of “stereoisomers” and only for Schedule I. The CND adopted by vote the WHO recommendation, and according to the OLA document “there is no record of any action taken with respect to the substances to which WHO objected”. And indeed, correctly following treaty procedures no vote was taken on the Spanish proposal because that included a much broader range of substances that the WHO had not recommended for international control.
The Netherlands argued at the time that the 1971 Convention “prescribes that new substances should first be carefully examined by WHO and then could be added to one of four Schedules if deemed necessary” and that the Spanish proposal therefore “may contradict the scheduling procedure”. The Netherlands “attaches great importance to a balanced and thorough expert opinion on health and social risks created by new substances before they are included in a schedule. As indicated above, WHO is required by the Convention to examine and evaluate each individual substance. Applying unconditional analogue scheduling would, however, substantially diminish the importance of this WHO task. In the opinion of the Netherlands, this would be a loss of expertise and negatively affect the scientific basis of the decision-making process within the Commission on Narcotic Drugs.”
As the OLA opinion confirms (in spite of its confused wording), there is not a single precedent in the history of scheduling decisions under the 1971 Convention where the CND decided to schedule a substance that had not been recommended for scheduling by the WHO. If the CND would decide to vote on the Chinese proposal to schedule ketamine, despite the fact that the WHO has already determined three times that it does not meet the threshold criteria for international control, it would therefore set a very worrying precedent. It effectively means the removal of the medical/scientific threshold for international control and abolishing the determinative nature of the mandate given to the WHO. The consequence of that for the future would be that any CND Member State from now on can call for a vote to put any substance on whatever schedule of the 1971 Convention (under the 1961 Convention this would be unthinkable), regardless of the opinion of the WHO Expert Committee. Tramadol and khat would be likely candidates to become scheduled in the coming years in a similar way, using the ketamine precedent to justify neglecting WHO’s expert advice again.
The OLA opinion was accompanied by a disclaimer saying that countries and the CND “may take a different view to the responses we provide. As such, our response should not in any way be construed as the only or definitive view.” Countries should critically examine OLA’s legal opinion and carefully consider its consequences for the future functioning of the UN drug control treaty system. Allowing the CND to vote about the scheduling of ketamine contrary to WHO’s recommendation, makes a mockery of the evidence-based intentions of the treaties and politicizes scheduling decisions in the future. Countries that are genuine in their calls for a more health- and human rights-based drug control system, for improving access and availability of essential medicines and for a more evidence-driven drug policy making, cannot allow this to happen…


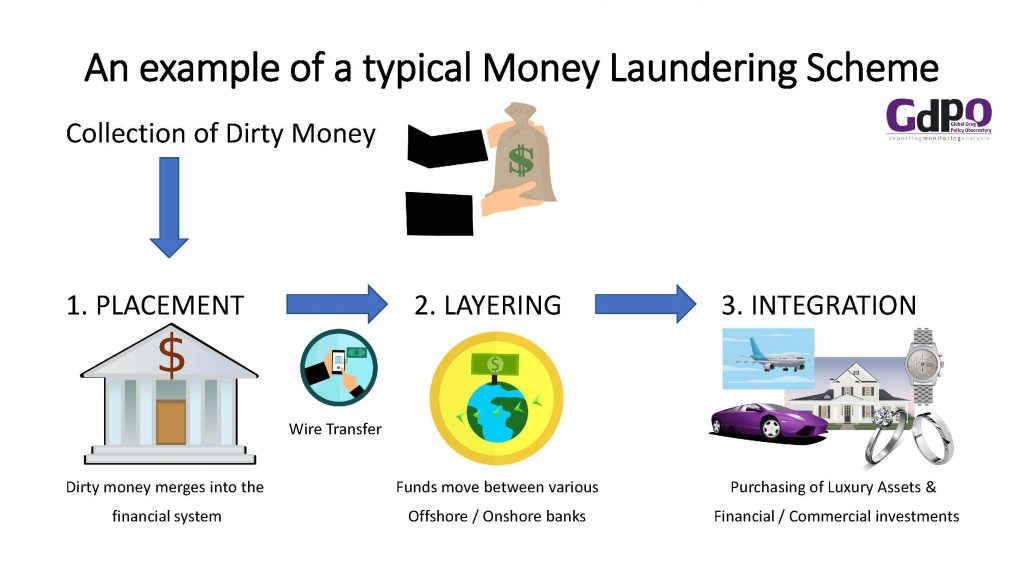








 The Commission on Narcotic Drugs (CND) in Vienna will decide next week between two opposite proposals by China and the WHO about international control of
The Commission on Narcotic Drugs (CND) in Vienna will decide next week between two opposite proposals by China and the WHO about international control of